
Gatekeepers of Information
Orthopedic Business Review
written by Will Kurtz, M.D.
November 13, 2020

Tech Theme - the Disruption of Gatekeepers
Gatekeepers historically control the flow of ideas and products between producers and consumers. Simultaneously developing both the producer and consumer side of a marketplace is hard and prevents new companies from entering a marketplace until a new method of distribution provides a novel way for innovative companies to connect consumers and producers. This disruptive process has been well characterized by Clayton Christenson in the Innovator’s Dilemma.
Rich Barton (Founder of Expedia, Glassdoor, and Zillow) describes how the internet has disrupted gatekeepers as “Power to the People” on the latest “Invest like the Best” podcast.
Historical Examples of Gatekeeper Disruption
The printing press (invented in 1440 by Johannes Gutenberg) allowed wide distribution of the bible. On October 31st, 1517, Martin Luther famously nailed his Ninety-five Theses to the door of All Saints' Church in Wittenberg which started the Protestant revolution. The Protestant revolution was made possible by the use of written text as a new method of distribution of the Christian faith.
The three major broadcast TV networks (ABC, NBC, CBS) were the gatekeepers for all information until cable companies introduced 100’s of niche news channels with 24 hour a day news coverage. Broadcast networks still required all viewers to watch the only one show per channel at any one time (one to many relationship). Netflix, Hulu, and YouTube’s streaming service (one to one relationship) further disrupted the temporal restriction of broadcast networks by providing thousands of different shows on one channel at any time.
Newspapers’ editorial boards controlled all the news that was fit to print (Overton Window) until Twitter and Facebook allowed anyone to instantly publish a wide array of opinions without oversight or accountability. The newspaper’s one to many relationship that promoted a shared set of facts was disrupted by Facebook’s one to one relationship that promotes a unique, personalized set of facts.
Other gatekeepers that have been disrupted include travel agents (Expedia), real estate agents (Zillow), taxis (Uber), and AAA (Google Maps),
The effects of disrupting gatekeepers
The above examples show new methods of distribution (i.e. the internet) resulting in the disruption of traditional gatekeepers, but is disrupting gatekeepers good or bad for society? The answer is that it depends. Oppressive Arab dictators were gatekeepers of the news until Twitter allowed for citizens to share information directly in the Arab Spring. The removal of dictators acting as oppressive gatekeepers and restoring power to the people is obviously a positive for society. Facebook’s disrupting the newspaper’s editorial board as a gatekeeper of news has allowed for the proliferation of fake news, echo chambers, and content bubbles which has divided our society.
Unfortunately, a world without gatekeepers and limitless content has exposed flaws in human nature that are described by these tech themes that have been popularized by Tristan Harris.
Confirmation Bias - People naturally seek out content that confirms their preconceived beliefs and avoid content that challenges their opinions.
Sensationalism - Content producers have always had financial incentives to increase the consumption of their content. Newspaper have promoted sensational content over meaningful content as evidence by the popular quote, “If it bleeds, it leads.” The artificial intelligence deciding which piece of content to display in Facebook’s newsfeed has accelerated this sensationalism through its hyper-targeting and rapid feedback loops that show us more sensational content (i.e. click bait).
Anger & Fear over Love & Support - Harder emotions (like anger) drive engagement more than softer emotions (like love). Social media’s AI algorithms surface content that elicits these harder emotions because it keeps us engaged in their apps and increases their DAU (daily active users).
Content Bubbles - The personalization of content delivery through social media’s the one to one relationship means our society does not even share the same set of facts. Because I see one set of facts and you see another, we can’t even agree on what we should be discussing.
But could these tech themes affect healthcare? The anti-vaccination movement could be considering an example where social media has had a harmful effect on our society’s healthcare.
Gatekeepers in Healthcare
There are two types of gatekeepers in healthcare that we will discuss:
Gatekeepers to healthcare providers (HCPs)
Gatekeepers to patients
Gatekeepers to HCPs:
Medical Journal Editorial Boards
Healthcare journals (and committees that decide which research papers get on the podium) have historically been the gatekeepers of medical information between industry and healthcare providers. The editorial boards of a specialty’s main journals and meetings decide which articles are accepted for publication and presentation and thereby which procedures were discussed and adopted by providers. If a healthcare provider or company wants their procedure discussed and adopted, they have to set up a clinical trial, enroll patients, follow outcomes, write a paper, and get their research published. Getting an article published or podium time at a meeting often meant selecting an influential HCP to help design an implant or author their paper. These influential HCP often get selected for more industry consulting opportunities which in turn makes these HCP more influential which in turn makes them get selected for more consulting opportunities. Some new techniques like DAA apparently struggled to initially gain exposure through publications and meetings until the DAA trend was adopted by members of these editorial boards.
These editorial boards play an important role in ensuring the integrity of medical education. The internet’s disruption of editorial boards as the gatekeeper to the HCPs may lead to a harmful increase in biased content delivery. Hopefully, HCPs have the proper education to differentiate well designed studies from propaganda, but this trend could have harmful affects to healthcare.
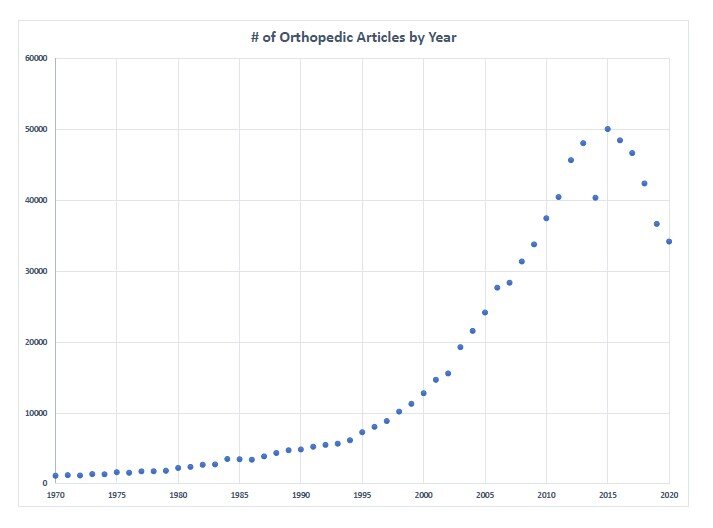
Number of google scholar articles that mention “orthopedics” by year
Similar to how cable companies offered more channels than broadcast TV, the number of medical journals has sky-rocketed starting around 2005. The electronic distribution of digital journals has lowered the cost to produce a journal. The increase in number of journal articles (shown in this graph) has been driven by the increase in niche sub-specialized journals. Comprehensive journals that discuss all aspects of a specialty have lost market share to niche journals that discuss only a sub-specialized area in much the same way as TV viewers have shifted away from ABC, NBC, CBS news and towards FoxNews and MSNBC. Physicians are now overwhelmed with potential articles to read and only have time to read the articles in their sub-specialized field. The abundance of content further pushes orthopedic physicians’ practices into further sub-specialization, which could have implications for surgeons taking general call.
Gatekeepers to Patients:
Healthcare providers have historically been the gatekeepers of medical information between industry and patients. The internet has changed that forever. Now, patients come into our office with stacks of research from websites. Google displays 67 million links for “non-operative cures from knee arthritis.” Every physician knows arthritis is treatable but not curable, so why does our society allow 67 million websites to claim the opposite (obviously not all of these sites claim to cure arthritis). Google is not the problem. Google has just crawled 67,000,000 websites that claim to cure arthritis, and there is little to no regulation (i.e. gatekeeper) to prevent these websites from luring in desperate patients with their false claims.
Empowering patients through legitimate medical education has definitely improved healthcare. I want my patients to be well educated about their disease. But what about the false claims that are designed to look like legitimate medical information? Can we expect an average reader who may be sick, elderly, or desperate to be able to differentiate a well-designed clinical study from unsubstantiated marketing material?

Traditional DTC Advertising
In 1997, the FDA started allowing pharmaceutical companies to advertising their products directly to consumer (DTC advertising). The public nature of TV (one to many relationship) means these ads are targeted at the general population and scrutinized by everyone. Our society and the FDA can regulate the claims made by these pharmaceutical ads because the ads are transparent and the pharmaceutical companies are accountable.
Social Media DTC Advertising
The secrecy of social media with its one to one news feed has been a breeding ground for confirmation bias, sensationalism and bubble formation in politics, and now in healthcare. The anti-vaccination movement was fueled by social media without oversight from the general population. Most HCPs probably did not click on the “click bait” about vaccines, and therefore HCPs were not immersed in this content bubble. There are books and Facebook groups titled “What your doctor is not telling you about …” How are the FDA and/or conscientious physicians supposed to prevent charlatans or snake oil salesman from selling their unproven products when there is no transparency or accountability in the social media ad world?
With Facebook’s artificial intelligence ad targeting, any business can display Facebook ads that sell their “snake oil” to users who are similar to that business’s previous customers. The artificial intelligence might learn that users who have previously clicked on the anti-vaccination movement will often buy “snake oil” while users who have a medical education or who work at the FDA will not. The AI algorithms may learn that certain genders, races, or education level are more susceptible to the false claims made by these charlatans and more willing to believe their unsubstantiated technologies. The Facebook’s ad algorithms can do the creepy things that most people would say are unethical. Because this ad targeting is happening without any transparency, our society looks the other way. The end result is that these charlatans are targeting our society’s most vulnerable users without any oversight from mainstream users. (Disclaimer: I can not prove that this AI ad targeting is happening in healthcare, but it definitely happens in other industries like politics)
Thankfully, on September 6, 2019, Google announced their healthcare advertising policy that “prohibits advertising for unproven or experimental medical techniques such as most stem cell therapy, cellular (non-stem) therapy, and gene therapy.” Facebook has recently stopped selling ads to the antivaccination movement, but more needs to be done by Facebook to protect our society’s vulnerable population.
How Social Media may affect HCPs

Could social media’s AI algorithms create bubbles among HCPs? It seems reasonable to accept that orthopedic surgeons and cardiologist don’t need to read the same journals, but these algorithms have the capability of getting more granular than just a HCP’s specialty. LinkedIn, Facebook or Doximity could easily index medical journals, learn what each HCPs click on, and then deliver similar articles that confirm what the HCP already believes. Would the social networks try to keep us reading the next article by only showing us articles that confirm what we already believe? Will article titles start to look like click bait (i.e. The worst surgical complication of my life was …) ? Could we see confirmation bias, sensationalism, and content bubbles in healthcare education? Could confirmation bias and content bubbles cause HCPs to not even agree on which medical information is relevant to discuss? If we consider how social media and AI algorithms have changed the delivery of our daily news, I think it is reasonable to assume this trend could happen to medical education.
Thought leaders and influencers have historically been the HCPs who speak on the podium and publish the journal articles. Historically, the only way to teach uninformed HCPs about a new technology was through publications and meetings. Obviously, the internet is slowly disrupting this bottleneck in the flow of information. These large orthopedic companies spend millions of dollars on industry meetings. It begs the question, is their marketing spend better utilized on a meeting or paying 100 orthopedic surgeons for every LinkedIn post about their product that receives more than 500 likes? Will we see the orthopedic surgeons with the most Twitter followers or LinkedIn connections get the most consulting contracts? Social media influencers like Kylie Jenner have used the internet (Twitter, Instagram, Facebook ) to bypass the traditional gatekeeper and directly interact with their fans. It is reasonable to assume HCPs will utilize the internet to bypass gatekeepers and distribute their content to willing consumers through social media (and stupid blogs/newsletters).
Regulation
Our professional medical societies need to act as gatekeepers and hold all HCPs to high ethical standards for content delivery including social media posts and websites. Social media companies need to provide accountability and transparency to healthcare advertising. The FTC and/or FDA should require that all healthcare advertisements including social media ads to be registered and available for public scrutiny. The FTC should enact serious fines for making false medical claims with a whistle blower program. We can not assume a desperate patient will have the ability to differentiate legitimate medical information from a charlatan selling the next fountain of youth.
Gatekeepers to medical care
Physicians have always been the gatekeeper to medical care. The above paragraphs discuss how information now flows directly to patients through the internet, but medical care has historically been a physical event that requires a patient to be seen by their HCP. The difference between patients researching their disease on the internet and patients receiving their care through a virtual visit on the internet is a fine line which is slowly being crossed. The medical community won’t realize how far we have crossed this line until we are looking in the rearview mirror. When medical care becomes virtual, this new distribution method will open up opportunities for outsider to disrupt physicians as the gatekeepers of medical care. This topic is complex, and we will drive deeper into this concept in another blog that will be published in a few weeks.
Conclusion
We can’t put the genie back in the bottle. The traditional gatekeepers are going to be disrupted and loss some of their influence. The flow of information on the internet is like a river. It will find the easiest and fastest path to its destination, which will have both positive and negative effects on our society. It would be foolish though to think that we can stop it.
In short:
Broad medical journals are being disrupted by niche medical journals (TV to Cable).
All medical journals are being disrupted by social media platforms (newspapers to Facebook).
Medical education may eventually become curated by AI algorithms which may have deleterious effects to medical education (content bubbles, sensationalism, etc.).
The lack of gatekeepers (editorial boards) may hurt the integrity of medical education and allow the propagation of mis-information.
Patients (and some HCPs) are vulnerable to mis-information; therefore we need transparency and accountable in social media.
The FDA and/or FTC need to regulate the medical claims made by all parties on the internet.
Influencers or thought leaders will expand from editorial boards to include social media influencers.
Additional Reading:
Previous Article - #1 - Introduction to Orthopedic Business Review
Next Article - #3 - The Paradox of Skill